
The optimal timing for this procedure is within a “golden” window of 3-5 months following the injury. This time frame ensures early and effective reactivation of paralyzed muscles, leading to muscle strength of grade 4.
The primary targets of surgery are restoring shoulder abduction and elbow flexion. The procedure is conducted under General Anesthesia, with patients admitted a day before surgery.
Routine blood investigations are performed, a pre-anesthetic check-up is conducted, and an informed written consent form is signed. In many cases, nerves are harvested from the leg to repair partial Brachial Plexus injuries. This procedure does not create any deficit in the leg, apart from mild sensory abnormalities in the outer aspect of the ankle region, which typically resolve over time.
a) Nerve Repair
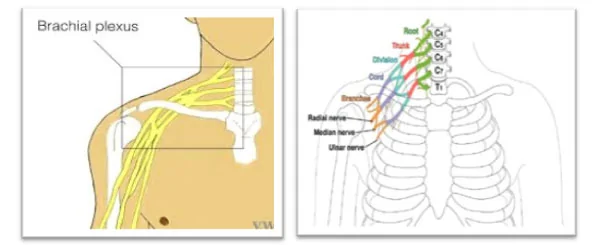
Nerve repair is performed in cases of nerve rupture. The Brachial Plexus is explored to identify ruptured nerves, remove scarred nerve segments, and repair the nerves using grafts harvested from various parts of the body. Nerve repair is usually possible in upper Brachial Plexus ruptures. An incision is made in the neck region above the clavicle, muscles are dissected, and nerves are explored.
Neuromas are excised, and nerves are repaired using grafts from the leg if the proximal nerve roots are healthy. Additionally, the spinal accessory nerve is transferred to the supra-scapular nerve to restore the initiation of shoulder abduction movement, a critical transfer in all Brachial Plexus Injuries.
 b) Nerve Transfer
b) Nerve Transfer
Nerve transfer involves intentionally dividing a physiologically active nerve (with minimal donor-related complications) and transferring it to a more important yet irreparable paralytic nerve of the Brachial Plexus.
- Oberlin I & II Method: (For Elbow Movement)
The most commonly used nerve transfer technique for elbow flexion in upper arm-type BPI is the Oberlin transfer. The biceps muscle, responsible for elbow flexion, is supplied by the musculocutaneous nerve. An incision is made on the inside of the arm, and nerves are explored. One or two nerve fascicles are taken from the ulnar nerve and directly joined with the motor branch of the biceps muscle of the musculocutaneous nerve (MCN).
-
Mackinnon’s Method: (For Shoulder Movement)
The preferred nerve transfer technique for shoulder abduction in upper arm-type BPI is the Susan Mackinnon method. The deltoid muscle, responsible for shoulder abduction, is supplied by the axillary nerve. An incision is made on the backside of the arm, and nerves are explored underneath the triceps and deltoid muscles. Nerve fascicles from the triceps nerve branch are taken and directly joined with the axillary nerve.



















")
")
")