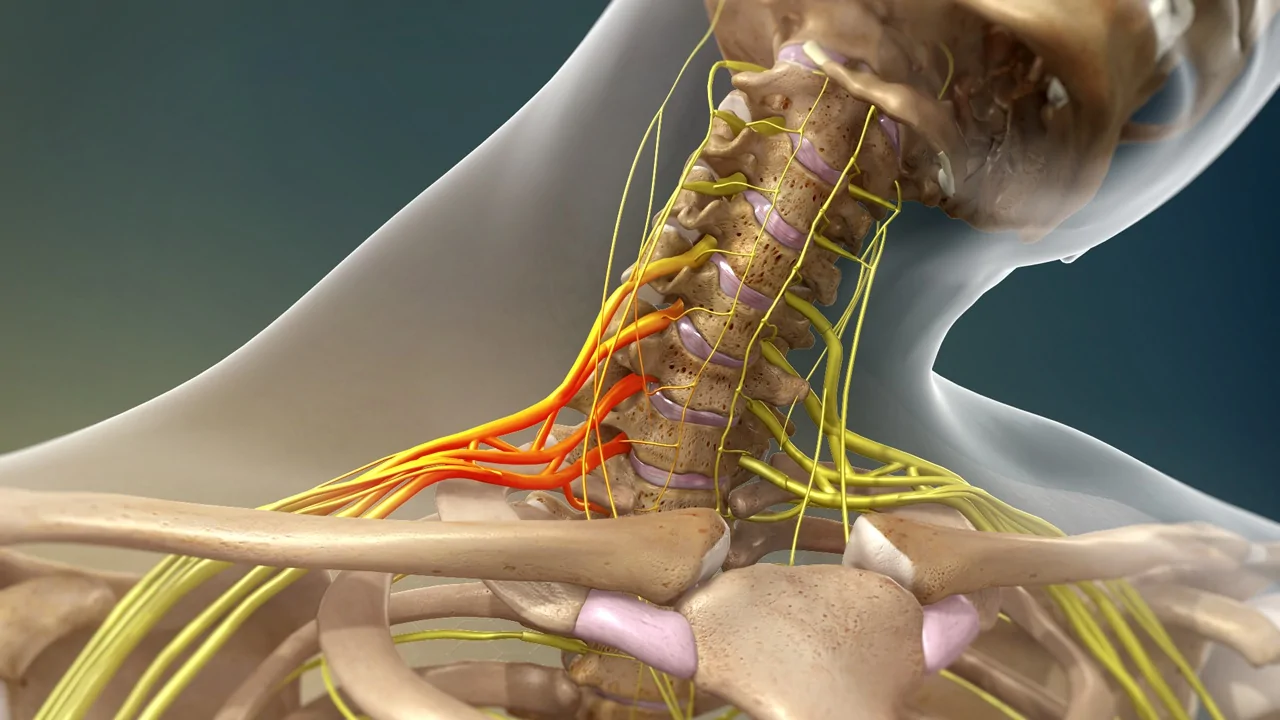
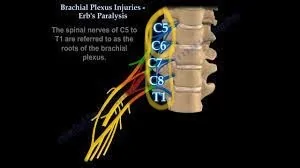
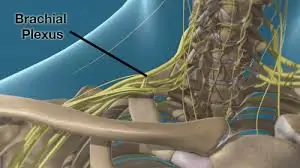
Brachial plexus injuries are closely associated with the brachial plexus, a network of nerves in the neck and shoulder region. Typically, complete brachial plexus injuries result from accidents where the arm is forcefully stretched or injured. These injuries involve the complete severance of nerve roots C5, C6, C7, C8, and T1 in the neck, leading to weakness, numbness, or loss of motion in the affected shoulder, arm, forearm, and hand.
Complete BPI — explained on video
Procedure explainers, surgeon Q&A, and patient stories — straight from Dr. Amit Agarwal.
This video is for educational purposes only.
Treatments are individualised according to each patient's condition and
needs. Similar results cannot be guaranteed for every individual.
Understanding a Complete Brachial Plexus Injury
Brachial plexus injuries are closely associated with the brachial plexus, a network of nerves in the neck and shoulder region. Typically, complete brachial plexus injuries result from accidents where the arm is forcefully stretched or injured. These injuries involve the complete severance of nerve roots C5, C6, C7, C8, and T1 in the neck, leading to weakness, numbness, or loss of motion in the affected shoulder, arm, forearm, and hand.
Impact of Complete Brachial Plexus Injuries
Complete brachial plexus injuries leave the limb entirely incapacitated. Individuals with such injuries cannot move, lift their affected shoulder, elbow, or wrist, and they lose all hand movements and the ability to grasp objects or sense anything in the affected limb. This injury is more commonly observed in men aged 15-25 years. Notably, upper brachial plexus nerves (C5, C6) are more prone to stretching or rupturing, while lower brachial plexus nerves (C8, T1) tend to avulse or detach from the spinal cord.
Immediate Actions for Suspected Complete Brachial Plexus Injuries
In the immediate aftermath of an accident, it is crucial to conduct a thorough examination of the patient to rule out fractures at the injury site or injuries to other body parts, such as the head, spinal cord, or chest. Assessing the patient’s level of consciousness and their ability or inability to lift the limb after the accident can provide valuable insights for later management. Addressing any limb fractures takes precedence before planning any surgery for Brachial Plexus Injuries. For more information on the causes, investigations, and the role and timing of surgery, please refer to our Brachial Plexus injuries page.
Surgery for Complete Brachial Plexus Injury
The timing of surgical intervention is critical in cases of complete injuries. The adage “sooner the treatment, better the outcome” holds true for brachial plexus injuries. Surgery involves exploring, repairing, and transferring nerves. In cases of sharp open injuries, immediate surgery is performed. In contrast, blunt closed injuries, which are more common, are observed for the first 2-3 months. This period allows for spontaneous recovery, if present. If no recovery is observed after three months post-accident, nerve repair or transfer surgery is conducted as soon as possible.
Significance of Timing in Complete Brachial Plexus Injuries
For injuries occurring within 9 months to 1 year, surgery is still a viable option, although the chances of recovery are somewhat diminished compared to surgeries performed within 3 months. However, after 1 year post-accident, attempts at nerve transfer surgery have shown very limited success due to insufficient time for nerve regeneration. In such cases, specific targeted muscle and tendon transfers are preferred over nerve transfer surgery.
Targeted Movements in Nerve Surgery for Brachial Plexus Injuries
During surgery for complete brachial plexus injuries, the focus is on restoring several essential movements, including shoulder abduction, elbow flexion, wrist extension, and some sensory recovery in the hand.
Comprehensive Restoration Through Staged Procedures
It’s important to note that a single surgery cannot fully restore all upper limb movements due to the limited availability of donor nerves. Achieving comprehensive recovery typically necessitates multiple staged surgical procedures to regain and target different hand movements.
Surgical Procedure for Nerve Repair/Transfer at Kayakriti for Complete BPI
The optimal timing for this procedure is within 3-5 months of the injury to reactivate paralyzed muscles effectively, leading to a strength level of grade 4.
This surgery is conducted under General Anesthesia, with patients admitted a day before the procedure. Prior to surgery, routine blood investigations are performed, a pre-anesthetic check-up is conducted, and an informed written consent form is signed.
In many cases, nerves are harvested from the leg to repair complete brachial plexus injuries. This procedure does not create any deficit in the leg, except for mild sensory abnormalities in the outer aspect of the ankle region, which tend to subside over time.
Nerve repair is employed in cases of nerve ruptures. The brachial plexus is explored to identify ruptured nerves, remove scarred nerve segments, and perform nerve repair. In upper brachial plexus ruptures, nerve repair is feasible, as the lower trunks are avulsed from the spinal cord, making nerve repairs impossible.
The procedure typically involves an incision in the neck region above the clavicle. Muscles are dissected, and nerves are explored. Neuroma is excised from the upper brachial plexus, and nerve repair is accomplished using nerve grafts from various parts of the body. Additionally, the spinal accessory nerve is transferred to the suprascapular nerve to restore the initiation of shoulder abduction movement, a vital transfer in all Brachial Plexus Injuries.
Nerve transfer is a surgical option that intentionally divides an actively functioning nerve (with minimal donor-related complications) and transfers it to a more crucial yet irreparable paralytic nerve of the brachial plexus.
Intra-plexus nerve transfer is typically applied in cases of nerve avulsion from the spinal cord, where at least one spinal nerve has experienced rupture but is still suitable for transfer. These transfers are not returned to their original pathway but redirected to more critical nerves. The choice of intra plexus nerve transfer is personalized, depending on intraoperative findings, the surgeon’s approach, and the patient’s specific condition and requirements.
Extra Plexus nerve transfer entails transferring a neighboring nerve (either from the same or opposite side of the neck) to the avulsed brachial plexus, facilitating the negotiation of a paralytic nerve. Commonly used donor nerves are primarily aimed at motor re-innervation, including the phrenic nerve, spinal accessory nerve (accessed via an anterior neck approach), deep motor branches of the cervical plexus (cervical motor branches; CMBs), hypoglossal nerve (XII), contralateral C7 (CC7) spinal nerve, and intercostal nerves. Extra Plexus sensory nerve transfer, such as supraclavicular sensory nerves to the median nerve transfer, is occasionally employed to restore sensation to the paralytic hand.
a) Nerve Repair
b) Nerve Transfer
Intraplexus (Within the Brachial Plexus) Nerve Transfer
Extra Plexus (Outside the Brachial Plexus) Nerve Transfer
Recovery After Brachial Plexus Surgery
Brachial plexus neurotization procedures are lengthy surgeries, typically lasting a minimum of 6 to 8 hours.
After surgery, patients usually spend 2 days in the hospital before being discharged.
Non-dissolvable sutures are removed after 14 days.
Subsequently, regular monthly follow-up examinations are mandatory to assess the progress of nerve repair and nerve regeneration.
Results Following Surgery for Complete Brachial Plexus Injuries
The outcomes of nerve repair surgery for complete injuries are frequently incomplete and can vary significantly. These outcomes hinge on various factors such as age, weight, co-existing medical conditions, and the time elapsed since the accident.
The best possible result that patients can achieve, with dedicated effort and physiotherapy, in the case of complete brachial plexus injury includes the ability to:
These improvements enable individuals to use their paralyzed hand as a supportive hand. It’s important to understand that nerve regeneration occurs gradually, at an approximate rate of 1 mm per day. Recovering from a brachial plexus injury is a time-intensive process, with patients often not experiencing significant results for several months, even after a successful surgery.
Abduct (lift the arm away from the body) the arm up to 90 degrees.
Flex the elbow (bend the elbow towards the body).
Achieve a mild grip in the hand (sufficient for holding objects).
Attain mild to moderate sensory recovery in the hand to prevent injuries or burns.
Postoperative Care and Rehabilitation
Following surgery for brachial plexus injuries, patients are advised to undergo regular physiotherapy and Transcutaneous Electric Nerve Stimulation (TENS) therapy. Maintaining a positive mindset and having the support of family, friends, and healthcare professionals are essential components of recovery and rehabilitation.
Addressing Incomplete Results After Surgery
Complete recovery after surgery for brachial plexus injuries can be unpredictable. Even in the best medical centers globally, success rates hover around 50% to 60%. In cases of incomplete recovery or when specific functions need to be regained in the arm, patients may require additional surgeries in the future.
Management Beyond One Year After the Accident
If more than one year has passed since the accident, it is advisable to consider muscle or tendon transfers for Complete Brachial Plexus Injuries (C5678T1) . This approach helps optimize functional restoration when the window for nerve repair or transfer has closed.
Less Than 1 Year of Injury – Partial Brachial Plexus Injury (C56 or C567)
More than 1 Year of Injury – Partial Brachial Plexus Injury (C56 or C567)
New section
New section
See the difference
Pre & Post Operation — Complete BPI
Real patient recovery — pre-operation on the left, post-operation on the right. All videos shared with patient consent.
Patient 1
Pre OperationPost Operation
Patient 2
Pre OperationPost Operation
Images shown are intended to provide general treatment insight only.
Every patient is unique, and outcomes may vary depending on individual
condition and treatment plan.
Common questions
Frequently asked questions
What is a Brachial Plexus Injury (BPI), and how does Kayakriti Clinic specialize in treating individuals with BPI within the first year of their injury?
BPI is a nerve injury in the brachial plexus, which can lead to arm weakness or paralysis. Kayakriti Clinic specializes in diagnosing and treating BPI cases that have occurred within the first year of injury.
What are the common causes of Brachial Plexus Injuries in individuals with injuries less than one year old, and how can these injuries be prevented?
Kayakriti Clinic can provide information about common causes of BPI, such as trauma or accidents, and discuss preventive measures to reduce the risk of such injuries.
How does Kayakriti Clinic diagnose Brachial Plexus Injuries in individuals who have recently experienced them, and what diagnostic methods are used?
Kayakriti Clinic employs advanced diagnostic techniques, including physical examinations and imaging studies like MRI, to accurately diagnose Brachial Plexus Injuries in individuals with recent injuries.
What are the available treatment options at Kayakriti Clinic for individuals with Brachial Plexus Injuries within the first year of their injury?
Kayakriti Clinic offers various treatment options, including nerve repair and transfers, to address Brachial Plexus Injuries in individuals who have been injured within the first year. They can explain the potential benefits of these treatments.
How crucial is early intervention for individuals with Brachial Plexus Injuries within the first year of their injury, and what are the expected outcomes?
Kayakriti Clinic can emphasize the importance of early intervention and provide insights into the expected outcomes and potential for functional recovery when treatment is initiated promptly.
What does the rehabilitation process entail for individuals undergoing treatment at Kayakriti Clinic for Brachial Plexus Injuries within the first year of their injury?
Kayakriti Clinic can describe the rehabilitation process, including the types of therapies and exercises involved in helping individuals regain arm function.
Real stories
What our patients say about Kayakriti
★★★★★
"Kayakriti Plastic Surgery & Dental Clinic is one of the best clinics — excellent doctors and a very professional team. The clinic is clean, well-maintained, and uses advanced technology. Doctors explain everything clearly and make you feel comfortable throughout the treatment. Highly recommended for both plastic surgery and dental care."
★★★★★
"My big brother had a critical accident in August 2025 — his right foot was injured badly. Thanks to Dr Amit, the plastic surgery was a great success and now he is walking on his feet. Dr Amit is polite, humble, and guided us like family."
★★★★★
"Dr Amit Agarwal is really a very good plastic surgeon — he operated on my leg. The treatment is really very good and the staff behaviour is very nice."
★★★★★
"Dr Amit Agarwal performed surgery for diabetic foot on my father. We were very troubled before going to him; after his treatment the condition is much better. He debrided all the infection and did grafting on the same."
★★★★★
"Dr Amit Agarwal operated on my patient for a congenital defect. A renowned plastic surgeon of Uttar Pradesh with excellent post-operative results. He explains every step of the treatment very nicely and is very determined towards his work."
★★★★★
"Dr Amit is very approachable, so it is easy to talk to him and ask all our queries. Before operating he explains the entire process with all the pros and cons. His staff is well-trained and well-behaved — I had a wonderful experience."
★★★★★
"Dr Amit Agarwal operated on my sister who got burnt two years back, leaving burn scars in her neck area. With the help of tissue expanders he has cured her scars to the utmost. Thank you sir for the treatment."
★★★★★
"Dr Amit Agarwal operated on my child for a congenital defect and has delivered brilliant results. We are completely satisfied with his treatment and recommend him to everyone."
★★★★★
"I consulted Dr Amit Agarwal for my son's gynaecomastia operation. His results have been very good — now my son is much more confident and comfortable with his looks after the operation."
★★★★★
"Dr Amit operated on my patient for a lip augmentation surgery to give her lips a proper cosmetic shape. The post-operative results are very good — she is very satisfied."
★★★★★
"Dr Amit Agarwal operated on my son for gynaecomastia. Due to the puffiness in his chest he felt very embarrassed in public. Thanks to Dr Amit's treatment my son feels much better aesthetically and has gained a lot of confidence about his looks."
★★★★★
"We consulted Dr Amit for cosmetic correction of my daughter's facial profile. He brought her upper jaw forward, surgically improving her appearance. It was a tough operation but the results are phenomenal — we are really satisfied with the look now."
★★★★★
"My son had his fingers joined since birth, causing a lot of functional problems. Dr Amit Agarwal performed syndactyly release on him. Now he is much better and there were no issues regarding post-operative complications."
★★★★★
"I got my rhinoplasty done under Dr Amit. The shape of my nose wasn't nice and my facial profile was getting hampered. Dr Amit elevated my nose to give it proper shape — now it is looking fine and I am very satisfied."
★★★★★
"Dr Amit Agarwal operated on my patient for deformed lips. He gave my patient a very aesthetic appearance and we are highly satisfied by the surgery. The cosmetic correction was successful with no complications."
★★★★★
"Dr Amit Sir is really a very good plastic surgeon — great nature, very cooperative staff, excellent scope for cosmetic treatment. Very happy and satisfied with the treatment. It really changed my life and enhanced my confidence."
★★★★★
"Dr Amit Agarwal performed cosmetic surgery on my nephew, who was facing a lot of issues with confidence due to gynaecomastia. After Dr Amit's treatment he is much better and has a boosted confidence level."
★★★★★
"I met a road accident two months back and my ring finger fractured. My orthopaedic doctor recommended Dr Amit for the joint fracture management. After he operated, my condition is much better."
★★★★★
"Dr Amit Agarwal operated on my patient for vascular malformation. He removed the complete swelling through an operation which went well and the results are good. The staff kept us well informed at every step and the whole process went smoothly."
★★★★★
"My patient wasn't satisfied with the aesthetic appearance of her lips. Dr Amit performed a lip augmentation surgery — it made her lips look more full and richer. She is very satisfied with the results."
★★★★★
"We were very troubled after my son met a road accident in which his jaw got fractured. Dr Amit confirmed the diagnosis quickly and proceeded for the surgery — through plating he joined the bones of the jaw and stabilised it. The condition now is much better."
★★★★★
"My brother is diabetic and hurt his leg; the wound was not healing for a long time. Dr Amit debrided all the infected part and covered it with a flap. The wound is now healed — we are lucky we got the correct treatment on time."