Understanding Partial Brachial Plexus Injuries
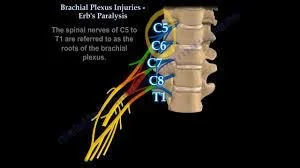
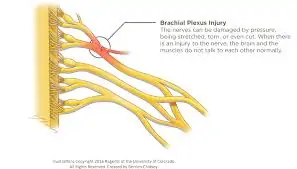
Partial Brachial Plexus Injuries involve the injury of C5, C6 nerve roots with or without C7 nerve root in the neck, leading to weakness, numbness, or loss of movement in the affected shoulder and elbow. Hand function remains good in cases of partial Brachial Plexus injuries. Deficits include shoulder stability, abduction (outward movement), external and internal rotation, elbow flexion (inner bending of the elbow), and forearm supination (rotating the forearm outward). If C7 is involved, there may also be variable weakness in the extension of the elbow, wrist, and fingers (straightening of elbow, wrist, and finger joints). This type of injury is often seen more frequently in men aged between 15-25 years.