Introduction
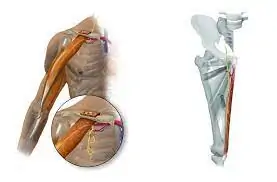
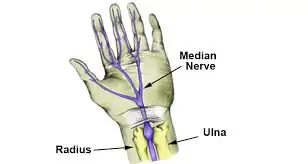
In the intricate landscape of our hands, nerves play a pivotal role in providing sensation and guiding our every movement. The median, radial, and ulnar nerves are vital components of the arm, ensuring that our hands function seamlessly. When these nerves face injuries or paralysis, it can lead to significant challenges and discomfort.