Obstetric Brachial Plexus Injury (OBPI)
Obstetric Brachial Plexus Injury (OBPI)

Obstetric Brachial Plexus Injury (OBPI)
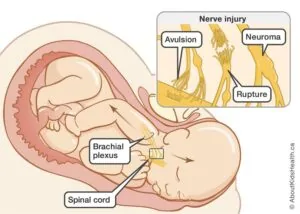
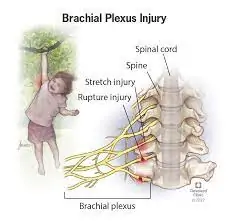
Obstetric Brachial Plexus Injury (OBPI), also known as Birth Brachial Plexus Injury (BBPI), refers to the paralysis of one arm from the neck down in an infant shortly after birth. This condition occurs due to an injury to the Brachial Plexus while the baby passes through the birth canal.
How Common Is OBPI?
Unfortunately, OBPI is relatively common among newborn children, with an incidence rate of 0.38 to 1.56 cases per 1000 live births.
Diagnosing Brachial Plexus Injury in Newborns
Following birth, newborns are routinely examined by pediatricians in hospitals. Any loss of movement in the arm or hand is identified and monitored. If arm palsy is detected, parents are advised to consult a Plastic surgeon for confirmation of the diagnosis and potential early intervention.
Challenges in Detecting Brachial Plexus Injury in Newborns
In rural areas where immediate post-birth evaluations are not feasible, arm paralysis in children with BBPI often goes unnoticed initially by parents. As the child grows and experiences difficulty performing normal hand functions, they are taken to a physician. Due to a lack of awareness, even healthcare professionals may fail to refer the child to the appropriate specialist promptly, leading to delayed intervention and suboptimal outcomes.
Risk Factors for BBPI
Several risk factors increase the likelihood of a child developing BBPI, including:
- Large-for-Gestational-Age Infants (Big Baby)
- Multiparous Pregnancies
- Previous Deliveries Resulting in Brachial Plexus Birth Palsy
- Prolonged Labor
- Breech Delivery (Feet First)
- Assisted Delivery (Using Vacuum or Forceps)
- Difficult Deliveries
Spontaneous Recovery in BBPI
Yes, spontaneous recovery is possible in cases of BBPI. Although some children experience natural improvement, there remains a subset of children who do not recover and require primary or secondary surgical intervention.
Types of BBPI
Obstetrical brachial plexus palsies are categorized into two major types based on the extent and severity of the injury:
Upper Brachial Plexus Palsy (“Erb’s Palsy”) – Involving the C5 and C6 nerve roots and sometimes C7 as well. This condition results in no movement at the shoulder and elbow joints but normal hand grip function.
Complete Brachial Plexus Palsy – Involving all nerve roots from C5 to T1, leading to a complete lack of movement at the shoulder, elbow, and hand, along with complete sensory loss.
Signs & Symptoms of Brachial Plexus Birth Palsy
- Full or partial lack of movement in the shoulder, elbow, and hand.
- Weakened hand grip.
- Numbness or decreased sensation in the affected upper limb.
- Abnormal positioning of the arm and hand, often with the arm bending toward the body or hanging awkwardly.

Management Within 2 Years of Birth
Is Early Intervention Required?
In most cases, babies with a brachial plexus injury regain some or full movement in the affected arm. Mild cases may improve without treatment. However, the concept of “wait and watch” has been replaced with early intervention to achieve better outcomes. Early intervention has proven to be more effective, aligning with results observed in adult patients after injury.
Planning Treatment for BBPI
- If a baby is brought to a specialist within 3 months of birth with arm palsy, a clinical examination is conducted to assess shoulder, elbow, and hand movements. If no movement is observed at the elbow by 3 months of age, parents are counseled about the possibility of surgery around 6 months of age. Surgeons prefer not to operate on infants at 3 months and recommend waiting until the child reaches 6 to 9 months of age.
- For babies brought to specialists within the first year of birth and who lack elbow flexion, nerve transfer surgery is advised. While surgery on such young children is a sensitive issue for parents, it is considered the best option if the child hasn’t shown any movement improvement by 6 to 12 months of age. However, the results of nerve transfer surgery vary among children, and it cannot guarantee the level of arm function post-surgery.
- If the child is brought for evaluation between 1 and 2 years of birth, nerve surgery can still be attempted within the first 2 years of birth.
Differences in Nerve Surgery for BBPI Compared to Adult Brachial Plexus Injury
Nerve repair outcomes in children differ from those in adults. Paralysis in children due to obstetric causes is usually not complete, with some fibers undergoing reinnervation due to neuromas crossing and resulting in minimal muscle activity. This innervation keeps the muscles viable and suitable for later nerve surgery.
Options for Nerve Surgery in Children with BBPI
Nerve surgery in children with BBPI typically involves two main approaches:
Nerve Repair with Nerve Grafts: Using a nerve from another part of the body (usually the back of the foot and leg) to patch an injured nerve in the brachial plexus.
Nerve Transfer: Connecting a healthy nerve outside the brachial plexus or an intra-plexus functioning nerve to the nerve whose function needs to be restored. Nerve transfer has the advantage of facilitating faster muscle reinnervation.
Nerve Surgery in Global BPI and Partial BPI
- In global palsy, where the entire brachial plexus is affected, surgical exploration involves identifying ruptured nerves, removing scar tissue from the nerves, and performing nerve repair using grafts from the leg. In cases where proximal nerve roots are unhealthy, nerve transfers such as intercostal nerve or C4 nerve transfers may be performed.
- In partial C5–6 or C5-6-7 palsy, where elbow flexion and shoulder abduction are affected, nerve transfers are aimed at regaining both of these movements. Procedures like the Oberlin transfer for biceps recovery and spinal accessory nerve (SAN) to suprascapular nerve (SSN) transfer for shoulder movement (infraspinatus and supraspinatus muscle function) are commonly employed. Additionally, transferring a nerve supplying one of the triceps’ heads to the axillary nerve can improve shoulder abduction.
Recovery After Nerve Surgery for BBPI
- After surgery, the child is closely monitored for about a week and then discharged.
- Dressings may be changed once or twice during this period.
- Parents are advised to schedule a follow-up appointment for suture removal after one week.
- Physiotherapy is recommended approximately one-month post-surgery, with follow-up appointments occurring monthly initially for recovery assessment, later reducing to every 3 to 6 months.
- Nerve regeneration is a gradual process, occurring at a rate of around 1 mm per day. Thus, parents are encouraged to ensure their child receives regular physiotherapy for the best outcomes.
Late Presentation of Brachial Plexus Birth Palsy
Should Late Nerve Surgery Be Considered for Children Older Than 2 Years?
- If the child is brought to us late after 2 years of birth, then the results of nerve transfer surgery are not good and fruitful.
- The child is allowed to grow, is closely evaluated at an interval of 3 to 6 months regularly and any signs of recovery are monitored. The child will eventually get a few movements back in his arm, forearm, and hand but will have multiple residual deformities due to cross innervation to different muscles which would require attention and surgeries in his/her life during growing years.
Why is the spontaneous recovery of muscles inadequate in BPBP?
Brachial plexus birth palsy injuries are usually low-velocity injuries. Injuries are either nerve rupture or in-continuity injuries but nerve avulsions from the spine are rare. The distance between the injured nerve ends is small in children after an injury during birth and hence reinnervation occurs leading to misdirected cross-innervation of fibres. This results in inadequate recovery of muscles and co-contractions.
What are co-contractions? And how do they affect the movements of the arm in a child?
Some muscle groups recover earlier than their antagonists and the unopposed action of these muscles combined with co-contractions could result in no action at the joints and contractures.
The result is-
a) inadequate functional range of moments and
b) deformities at various joints which are initially correctable but can lead to fixed
contractures if not corrected.
How are various deformities arising from BPBP corrected in a child?
A) Shoulder Deformities –
- If there is less movement of the shoulder outward (abduction)- If the muscles responsible for adduction of the arm are tight and the muscle responsible for the movement of the shoulder outwards are intact, then surgical release of these tight muscles will help. If the muscles responsible for the movement of the shoulder outwards are paralyzed, then trapezius muscle transfer is done.
- If there is less movement of lateral rotation of the shoulder- The most common procedure done is the transfer of LD muscle which is situated at the back to the muscle responsible for rotating the shoulder externally.
- If both abduction and external rotation of the shoulder are less – A combination of both the procedures mentioned above is done in stages.
B) Elbow Flexion Deformity – This can be corrected by the serial casting of the joint.
C) Forearm Deformities – These can be either supination deformity or pronation deformity.
These deformities can be corrected by rerouting specific muscles and osteotomies.
D) Hand Deformities – Loss of wrist extension
These hand deformities can be corrected by tendon transfers.
E) Other Deformities – There could be other deformities as well in a child which can be corrected as per the requirement.
A True Devotion to Healing
Where Compassionate Care Meets Advanced Medicine, Guiding You on the Path to Recovery and Well-being.



Have any questions? Call us now!
Frequently Asked Questions
What is Obstetric Brachial Plexus Injury (OBPI) or Birth Brachial Plexus Injury (BBPI)?
OBPI or BBPI refers to a condition in which an infant’s brachial plexus nerves are injured during the process of childbirth. This can occur due to various factors, including shoulder dystocia or difficult deliveries.
What are the common signs and symptoms of OBPI/BBPI in newborns?
Newborns with OBPI/BBPI may exhibit weakness, limited movement, or paralysis in one arm. They might also display signs of discomfort when the affected arm is touched or moved.
What causes OBPI/BBPI during childbirth?
OBPI/BBPI can result from the excessive pulling or stretching of the baby’s shoulder during a difficult delivery. Risk factors may include macrosomia (large baby), maternal diabetes, or a breech presentation.
How is OBPI/BBPI diagnosed in newborns?
Diagnosis typically involves a physical examination by a pediatrician or neonatologist who assesses the baby’s arm movements and reflexes. Further evaluation may include imaging studies such as ultrasound or MRI.
What are the treatment options for OBPI/BBPI in newborns?
Treatment options vary depending on the severity of the injury. Mild cases may resolve with physical therapy, while more severe cases may require surgery to repair damaged nerves or muscles. Early intervention is crucial for the best outcomes.
What is the long-term prognosis for infants with OBPI/BBPI?
The prognosis varies based on the extent of the injury and the effectiveness of treatment. With early diagnosis and appropriate intervention, many infants with OBPI/BBPI can achieve near-normal function in their affected arm, although some residual weakness or limitations may persist.
How does Dr. Amit diagnose OBPI/BBPI in newborns, and what diagnostic tools are used?
Dr. Amit uses a combination of physical examinations and diagnostic tools like ultrasound or MRI to assess and diagnose OBPI/BBPI in newborns accurately.
His Credentials









Kayakriti in News
")
")
")
Kayakriti Plastic Surgery & Dental Center
D-43, Near Punjab National Bank, Rajajipuram, Lucknow, Uttar Pradesh – 226017, India